Potentiating New Neuropathic Pain Drugs from Cannabis
Potentiating New Neuropathic Pain Drugs from Cannabis
Sean Hall 1*MD (res), MDA, LTA
1Managing director, Medlab Group Pty Ltd.
*Corresponding Author:Sean Hall, Managing director, Medlab Group Pty Ltd, Tel: +61 411603378; Fax: +61 411603378
Citation: Sean Hall (2024)Potentiating New Neuropathic Pain Drugs from Cannabis. Arch Mol Med & Gen 4: 123.
Received: January 08, 2024; Accepted: January 29, 2024; Published: January 31, 2024.
Copyright: © 2023 Sean Hall, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Pain and cannabis are two complex and potentially emotive topics, used together they on the surface posit relief and normality to many. But this is simply not true. Pain is subjective, pain relief can be fleeting. Can cannabis be an effective and sustainable analgesic? Moreover, can cannabis be successfully used as an opioid alternative in neuropathic pain? The data is limited, but several companies are published in this area and their work demonstrates a strong positive signal. Providing a brief overview of the opioid problem, and cannabis, the author talks through his experience in prepping for a new drug applicant for a mixed cannabinoid targeting cancer-induced pain.
Background
Over the past several years cannabis has made headlines with promises of therapeutic relief for a vast number of conditions. Further, cannabis marketers have taken significant liberties with health claims and therapeutic promises to promote their products, with many offering no science or clinical work to demonstrate efficacy, let alone safety.
Regardless cannabis has attracted much attention as either an investment opportunity and/or a panacea for many chronic illnesses.
As such, it is worth noting that cannabis legislation is at best loose, allowing for sub-par products to enter the marketplace with little to no recourse.
Health claims, still today, are the domain of health regulatory bodies, such as the Australian Therapeutic Goods Administration (TGA) and the United States of America, Food and Drug Administration (FDA), or the European Medicines Association (EMA) to name a few.
At the time of writing, it is worth noting Jazz Pharmaceuticals (via their acquisition of GW Pharma) has 2 products approved across all three health regulators, Epidiolex a cannabidiol (CBD) isolate is the most notable, and the first to successfully gain FDA approval. It is also worth noting, no cannabinoid has been approved for neuropathic pain.
Beyond this, it is worth reminding the reader, that dronabinol, a synthetic form of delta 9-tetrahydrocannabinol (THC) known as Marinol and Syndros, as well as Cesamet have been approved for some time with established safety profiles.
Present Day
Pain is categorized as acute, chronic, breakthrough, and cancer related. Cancer-related pain is typically neuropathic (NCP) and the onset can be related to the cancer itself and/or treatments, such as chemotherapy. Prevalence estimates are high. (So Young Yoon, 2018) cites NCP does not usually respond to opioids and thus multifactorial therapeutic agents are required to reduce the pain burden and improve the patient’s quality of life (QoL).
Opioids are standard care, and whilst opioids come in different formats and strengths, for many patients’ opioids do not offer symptom relief. For others, opioids present a real concern about potential addiction.
These concerns stem from the alarming opioid abuse figures in the USA.
Understanding The Us Opioid Problem
The US has over the past several years had a sorted history fighting the known opioid problem. The US Centre for Disease Control (CDC) states:
- Between 1999-2021 circa 645,000 died from opioid overdosing, inclusive of prescription opioids,
- Between 2019–2021, the US recorded a significant increase in the use of any opioid, after new initiatives were introduced to reduce opioid prescriptions and “doctor-shopping” across the nation.
- In 2021, it was recorded that 220 people die each day (in the US) from opioid overdosing.
The CDC data shows that despite best efforts, public access to opioids has increased, further (Nabarun Dasgupta, 2013) cited street prices for “black market” opioids; a landmark publication demonstrating (back then) how inexpensive these drugs were.
Whilst this commentary is not a review of the US opioid crisis, the intent is to demonstrate that the overall awe of the problem is, for many individuals, healthcare providers, and health regulators, motivation to look for, and/or market pain medications that may offer a potential replacement to opioid therapy.
Understanding Cannabis
Cannabis is a plant from the hemp family, to which, today cannabis is a popular general descriptive term for products that have cannabinoid compounds such as CBD and or THC (as the most known) as either singular ingredients to a product or as a mix of cannabinoids.
Today cannabinoids are available from agricultural greenfield production, and greenhouses or lab-made synthetic production.
Fast track to the present day; depending on where you reside, cannabis access to professional and/or recreational markets may be available.
In the author’s opinion, this increased access has hindered the necessity for proper clinical work to establish safety, efficacy, and tolerability on a compound or mix of compounds claiming to offer health benefits.
During my time at Medlab Clinical Ltd, my team extensively researched cannabis which led to the final formulation of the NanaBis program, a patented, nanoparticle racemic CBD and THC future new FDA drug, targeting cancer-induced pain.
Early research indicated several significant issues in developing a cannabinoid future drug; some of these issues were critical flaws due to the botanical nature of the compounds and how they were agriculturally grown. These flaws/issues included:
- Due to the variability of the botanical compounds, high and variable levels of vermin control, moisture, minerals, fungicides, and bactericides were readily present.
- Crops from the same agricultural specialists had limited or redacted batch control records.
- Crops from the same agricultural specialists had no standardization process that would pass a drug application.
- Crops appeared to be harvested mid-life cycle to increase annual economic yields.
- Certificates of Analysis (CoA) were basic and did not provide fungicides or bactericides as per World Health Organization (WHO) standards.
- Good Manufacturing Practice (GMP) was lacking.
- Analytical methods for detection of cannabinoids were performed without controls.
- Oral bioavailability of cannabinoids was poor.
- Onset of action was highly variable.
- Meta-analysis at the time showed no obvious safety data for the use of cannabinoids in pain.
In addressing these critical issues, we undertook significant quality processes to standardize each agricultural batch, with multiple stops for validation via detailed analytic work, and in many cases, result confirmation by a third party.
More so, we placed significant focus on by-passing first-pass metabolism in efforts to improve bioavailability. The author notes, despite marketing efforts from cannabis-related companies, (Ce Wang, 2022) still today cites oral CBD bioavailability at circa 6%, whilst (Stephanie Lunn, 2019) cites THC bioavailability at circa 10-20% for fasting and circa 6% fed patients.
A nanoparticle delivery system was engineered, Nano Celle®, which allowed sub-micron particles of 38 nanometers (nm) in size to deliver a therapeutic dosage of 1.6mg CBD and 1.6 mg THC per dose actuation of 0.3mL to the oro-buccal membrane. Due to Nano Celle®, the NanaBis investigational drug could rapidly cross the buccal membrane and utilize the facial lymphatics for a rapid systemic response.
The NanaBis investigational drug was subject to various in vivo and in vitro work resulting in several published studies and conference presentations.
In a landmark study, conducted at Royal North Shore Hospital under Professor S Clarke, NanaBis showed in advanced cancer patients with intractable pain, significant improvements in pain reduction and quality of life, the biggest and most surprising outcome was for patients whilst on NanaBis, a significant reduction in morphine milli-equivalents (MMEQ), marking primary evidence for opioid sparring.
Secondary real-world evidence studies (RWE) were undertaken to extend our understanding of MMEQ reduction to real-world opioid sparring, whilst continuing to demonstrate pain and QoL improvements.
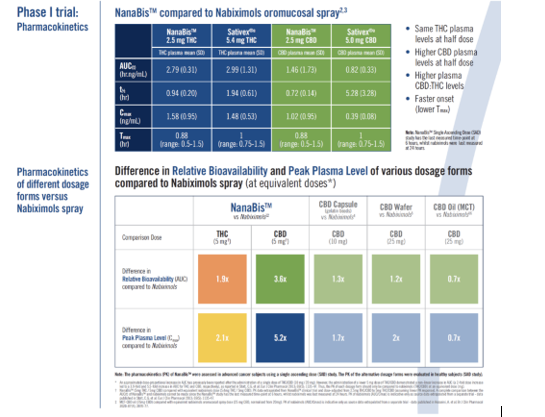
Pharmacokinetic work (Stephen Clarke, 2022) in an advanced cancer population showed the superiority of NanaBis over Nabiximols:
The RWE included some 1300 Australian patients with 15% of the group as cancer pain patients and 85% as non-cancer pain sufferers; over a mean intervention period of 5.5 months; marking the study as one of the only cannabis longevity studies ethically undertaken. Opioid sparring, improvements in pain, and improvements in QoL were again demonstrated across the group.
NanaBis was comprised of a 96% standardized botanical formulation performing within the prescribed 8% error margin. But the process for standardizing and manufacturing a precise medicine was both time and labor extensive.
In a review of the Sativex AUSPAR document and after consultation with the FDA, we decided to move to a synthetic version of the formulation. Working with a third-party collaborator we developed biosimilar FDA drug master files to eliminate any potential variation or contamination from the botanical compounds.
WHY GO TO ALL THIS WORK? In developing a drug, that is a substance that will produce a health benefit, several specific silos must be addressed:
- Precision – the formulation is exactly what you state it is, it will repeatedly deliver as you say it will deliver.
- Accuracy – everything can be independently confirmed, this includes analytic work, and this may mean new reference standards need to be created.
- Safety – a thorough body of work that proves safety, this includes safety packaging testing, through to the final formulation
- Efficacy – a thorough body of work that demonstrates efficacious dosing, side effects, and warnings.
- Tolerability – a thorough body of work that demonstrates the length of time a patient can safely and ethically stay on the product.
- Stability – the final presentation of the product undertakes rigorous testing in both accelerated and real-time format across different temperatures and humidity to force the degradation of the product over time, allowing for a specific understanding of the life of the viable product.
These elements, their process, and validation make up what is referred to as the product dossier inclusive of the Chemical, manufacturing, and Controls (CMC) package, used to evaluate the final drug application.
In my view, cannabis was not, is not a food or a nutraceutical supplement; the law (Australia) presently places cannabis under the TGA. Cannabis has many benefits; pain being the most notable, but as pain is subjective and has no prescribed pathology, cannabis companies must undertake rigorous study programs to fully understand the perceived formulations' performance in a condition that is complex and thwarted with co-morbidities and polypharmacy.
Disclaimer
Dr Hall is/was the CEO of Medlab Clinical Limited who owned and founded research into cannabinoids for the development of a future new drug application. Dr Hall is now the Managing Director of Medlab Group Pty Ltd, a private company involved in the licencing of Medlab technologies to third parties.